By Oliver Kim
I’ve written here before about areas where technology could play a role in providing access to complicated, controversial healthcare services. Earlier this year, I presented a forthcoming paper co-authored with a colleague on how technology can be used to provide greater equity in women’s health and how the law is being used to encourage such advances or block them. Given the political battles over women’s health, it should be no surprise that technology’s role in abortion access is under increasing scrutiny from lawmakers.
A medication abortion involves a two-step regimen: the woman first takes mifepristone, generally in a clinical setting, and 24 to 48 hours later, she takes misoprostol, generally in the privacy of her home. Recent research, though, suggests that women may not need to take mifepristone in a clinical setting: the World Health Organization revised its guidelines on whether the medications require “close medical supervision,” and a recent op-ed in the New England Journal of Medicine called on the Food and Drug Administration to revise its restrictions on mifepristone.
Given these findings, abortion providers have recognized that telemedicine could be utilized to expand access into areas where abortion services are limited due to geography, legal restrictions, or both. Since 2008, Planned Parenthood in Iowa has used telemedicine to overcome both provider shortages and geographic challenges: a physician can use video conferencing services to appear virtually at health centers across the state, reviewing a patient’s ultrasound and medical history remotely and providing counseling over a secure, private system. The majority of the medical literature finds that using telemedicine to provide medication abortions is just as safe and effective as if a woman met with a clinician in person.
As we discuss in our paper, when technology expands access to care that is politically controversial, policymakers may use the law to restrict such technological advances. In response to this use of telemedicine, states hostile to abortion began passing bans. When Iowa’s medical board attempted to restrict such a use of telemedicine, the Iowa Supreme Court struck down the board’s regulation, holding that it would be an undue burden on a woman’s right to an abortion. Some hailed the Iowa decision as groundbreaking and hopefully influential on other state supreme courts. (Later that same year, the U.S. Supreme Court in Whole Woman’s Health would strike down two Texas statutory restrictions on abortion providers as undue burdens on a woman’s right to an abortion.)
What I find interesting—and what came out after we submitted our paper—is how telemedicine and abortion are being treated in neighboring Kansas and how it reflects the larger legal debate over these issues. In 2011, Kansas first attempted to ban telemedicine abortions by requiring a physician to be physically present when administering mifepristone, thus eliminating the value of telemedicine. Subsequently, the Kansas state legislature modified the ban in 2015 by clarifying that a physician would not need to be physically present in a medical emergency; in 2018, the legislature passed explicit language in the Kansas Telemedicine Act that nothing in this new telemedicine legislation authorized the use of telemedicine for abortion. However, a Kansas court enjoined the Kansas attorney general, the only defendant in this line of cases, from enforcing this provision or the in-person requirements under the court’s prior 2011 decision.
Even more remarkable, in the same state that elected Sam Brownback governor twice, the Kansas Supreme Court recently held in Hodes & Nauser v. Schmidt that the Kansas constitution provided a fundamental right to an abortion.
Thus, it may seem surprising that in a subsequent decision, a district court refused to grant a preliminary injunction for Trust Women, a Wichita-based abortion provider, to prohibit the state from enforcing the telemedicine abortion restrictions. Part of this new case turns on standing as well as recognizing that the prior line of telemedicine-abortion cases only enjoined the state attorney general and was silent on whether the state health department or county attorneys were similarly enjoined from enforcing the telemedicine-abortion bans.
Further, the court also turned part of its decision on whether Trust Women would suffer an irreparable injury: the court found that there was insufficient evidence of an injury because Trust Women still required patients to be present physically at its Wichita clinic in its telemedicine pilot, and Trust Women had taken no preliminary steps to open clinics in remote rural parts of the state. Indeed, the court decried the prior telemedicine-abortion rulings as “a growing procedural backwater” and suggested that the court needs to be able “to resolve the underlying merits of the telemedicine abortion issue,” necessitating that “the parties… present additional evidence and more probing legal analysis than has occurred at this early stage.”
While the district court has significant discretion in considering a request for a preliminary injunction, it does feel troubling that the court suggests that Trust Women should have invested time and resources into a telemedicine strategy that might be illegal before seeking relief. In light of the bans and the legislature’s hostility, it seems unlikely that Trust Women could have raised the funds necessary to create a telemedicine infrastructure and build clinics in remote rural areas. After all, although the Kansas Supreme Court’s decision was not on the telemedicine restrictions, it seems unlikely that they would survive a strict scrutiny review under Hodes since the state will bear the burden of justifying the law. Moreover, it’s also likely that the restrictions might not survive review under Whole Woman’s Health given the weight of medical evidence that suggests singling out abortion from all other services provided by telemedicine, is suspect.
This is also playing out on the national stage as the Fifth Circuit in June Medical v. Gee seemingly sent a direct challenge to Whole Woman’s Health where the Fifth Circuit upheld Louisiana abortion restrictions that were basically identical to the Texas restrictions that were struck down. How June Medical is ultimately resolved will have ramifications for telemedicine in this particular context.
While medical evidence demonstrates that telemedicine is a safe means of providing medication abortion (as well as providing other benefits for women such as privacy), there are of course those that dispute this notion. One could see a conservative court finding that a telemedicine ban is not an undue burden: under the Trust Women preliminary injunction ruling, women in rural areas are no worse off than they were before since they never had access to abortion via telemedicine to begin with. Further, if waiting periods and similar barriers are upheld post-Whole Woman’s Health, this could put rural access even further at risk. In other words, a woman still has access to abortion, just not via telemedicine. Of course many such arguments could be applied to any telemedicine application, so the question turns back again: Why place restrictions just on abortion services?
In so many areas, though, telemedicine has been hailed as a way to increase access for all patients. The issues arise in the same areas where there have always been strong opinions, but the evidence and the trend lines are overwhelmingly in favor of expanded telemedicine access. The law should follow.



 Oliver is an adjunct professor with the University of Pittsburgh School of Law and a policy consultant in Washington, DC. He has over fifteen years of federal and state legislative and policy experience, including serving for eight years as a senior advisor to Senator Debbie Stabenow (D-MI) and two as deputy director for the Special Committee on Aging under Chairman Bill Nelson (D-FL). He was selected for the Woodrow Wilson foreign policy fellowship, the AcademyHealth Health Policy in Action award, the Hartford Foundation Change AGEnt program, and the American Council of Young Political Leaders’ international exchange program. He received his BA from Indiana University, JD from University of Minnesota, and LLM from the Georgetown University Law Center.
Oliver is an adjunct professor with the University of Pittsburgh School of Law and a policy consultant in Washington, DC. He has over fifteen years of federal and state legislative and policy experience, including serving for eight years as a senior advisor to Senator Debbie Stabenow (D-MI) and two as deputy director for the Special Committee on Aging under Chairman Bill Nelson (D-FL). He was selected for the Woodrow Wilson foreign policy fellowship, the AcademyHealth Health Policy in Action award, the Hartford Foundation Change AGEnt program, and the American Council of Young Political Leaders’ international exchange program. He received his BA from Indiana University, JD from University of Minnesota, and LLM from the Georgetown University Law Center.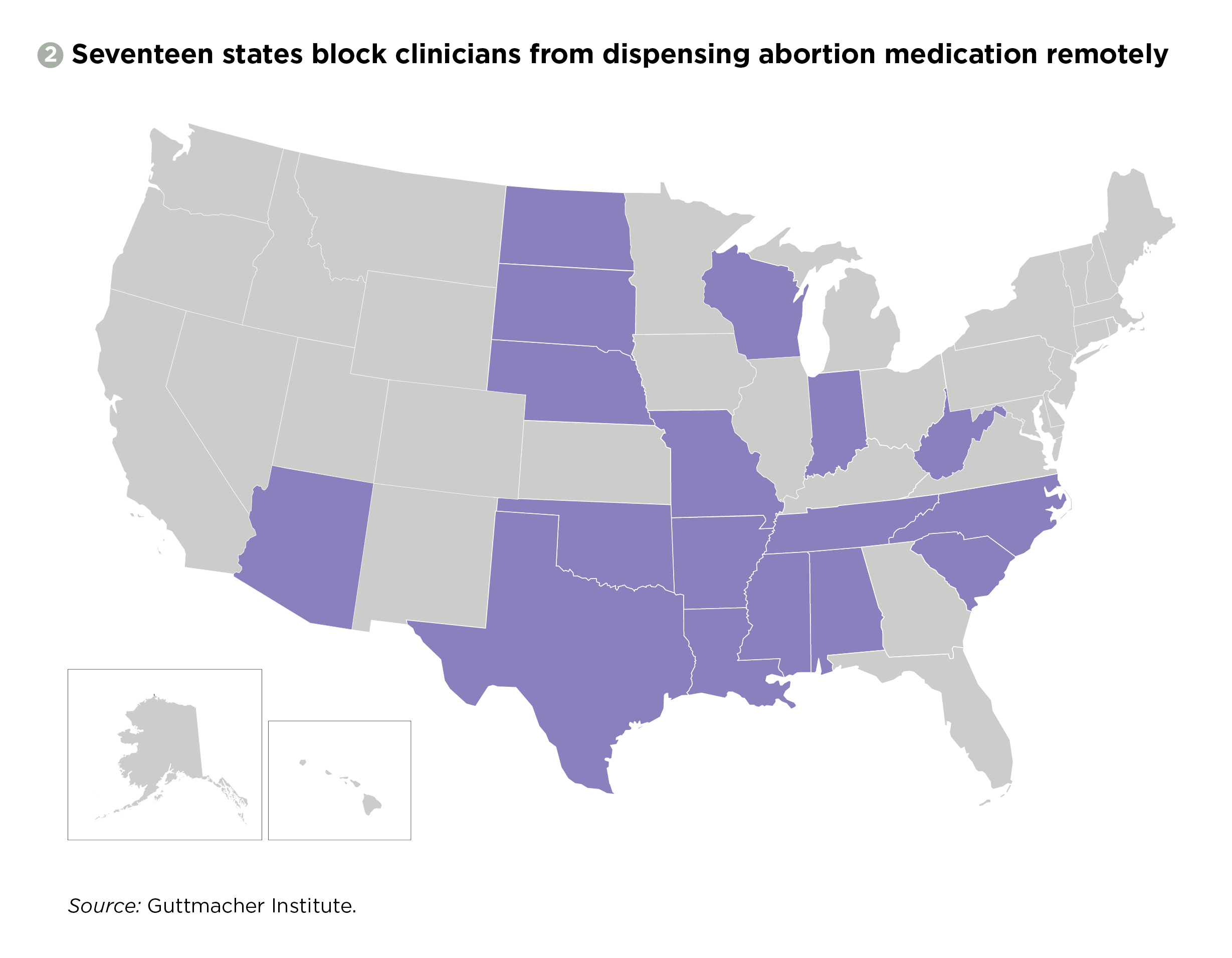{kind=link}
You must be logged in to post a comment.